Part One You will have two hours and 30 minutes to complete Part One.
1. A 3-year-old child with Down syndrome is admitted to the pediatric unit with asthma. The child doesn't enunciate words well and holds onto furniture when he walks. The nurse should ask the mother
A.how long the child has been like this.
B.if the child can walk without holding onto furniture.
C.how the child's condition today differs from his normal condition.
D.if the child always drools.
A B C D
C
Identify the chief complaint from how the child was previously behaving at home. Asking how long the child has been like this may be interpreted poorly by the caregiver. Focus on what the child can do--and not on what he can't do--to preserve the family's self-esteem. Focusing on negative aspects of the child's behavior is inappropriate.
2. A client who has received a new prescription for oral contraceptives asks the nurse how to take them. Which of the following would the nurse instruct the client to report to her primary caregiver?
A.Breast tenderness.
B.Breakthrough bleeding within first 3 months of use.
C.Decreased menstrual flow.
D.Blurred vision and headache.
A B C D
D
Some adverse effects of birth control pills, such as blurred vision and headaches, require a report to the health care provider. Because these two effects in particular may be precursors to cardiovascular compromise and embolus, the client may need to use another form of birth control. Breast tenderness, breakthrough bleeding, and decreased menstrual flow may occur as a normal response to the use of birth control pills.
3. The nurse is caring for a toddler in respiratory arrest. The nurse will assist with endotracheal intubation and use an uncurled tube because the
A.vocal cords provide a natural seal.
B.trachea is shorter.
C.larynx is anterior and cephalad.
D.cricoid cartilage is the narrowest part of the larynx.
A B C D
D
The cricoid cartilage in the toddler is the narrowest part of the larynx and provides a natural seal. This keeps the endotracheal tube in place without requiring a cuff. The vocal cords are narrower in an adult. The trachea is shorter and the larynx is anterior and cephalad, but these aren't reasons to choose an uncurled tube.
4. A client tells the nurse that she has been working hard for the last 3 months to control her type 2 (non-insulin-dependent) diabetes mellitus with diet and exercise. To determine the effectiveness of the client's efforts, the nurse should check
A.urine glucose level.
B.fasting blood glucose level.
C.serum fructosamine level.
D.glycosylated hemoglobin (Hb) level.
A B C D
D
Because some of the glucose in the bloodstream attaches to some of the Hb and stays attached during the 120-day life span of red blood cells, glycosylated Hb levels provide information about blood glucose levels during the previous 3 months. Fasting blood glucose and urine glucose levels give information about glucose levels only at the point in time when they were obtained. Serum fructosamine levels provide information about blood glucose control over the past 2 to 3 weeks.
5. Which of the following statements summarizes the underlying principle for the development of a parenbchild relationship?
A.The parents to-be had good role models in their childhood.
B.The relationship is part of the adult maturational process.
C.The development is directly related to the physical needs of the neonate.
D.The relationship is based on the need for early and frequent parent-infant contact.
A B C D
D
Early and frequent contact promotes love and satisfaction and can support the learned parental behavior that enhances parenting abilities and reduces ambivalence and feelings of resentment. Having good role models in childhood may be helpful but isn't the primary principle. Part of the adult maturational process excludes adolescents, who can form strong infant attachments. The relationship isn't directly related to the neonate's physical needs because human contact is needed for the infant to survive.
6. After striking his head on a tree while falling from a ladder, a young man is admitted to the emergency department. He's unconscious and his pupils are nonreactive. Which intervention would be the most dangerous for the client?
A.Give him a barbiturate.
B.Place him on mechanical ventilation.
C.Perform a lumbar puncture.
D.Elevate the head of his bed.
A B C D
C
The client's history and assessment suggest that he may have increased intracranial pressure (ICP). If this is the case, lumbar puncture shouldn't be done because it can quickly decompress the central nervous system and, thereby, cause additional damage. After a head injury, barbiturates may be given to prevent seizures; mechanical ventilation may be required if breathing deteriorates; and elevating the head of the bed may be used to reduce ICP.
7. When assessing a preschooler who has sustained a head trauma, the nurse notes that the child appears to be obtunded. Which of the following denotes the child's level of consciousness?
A.No motor or verbal response to noxious (painful) stimuli.
B.Remains in a deep sleep; responsive only to vigorous and repeated stimulation.
C.Can be aroused with stimulation.
D.Limited spontaneous movement; sluggish speech.
A B C D
C
The child is obtunded if he can be aroused with stimulation. If the child shows no motor or verbal response to noxious stimuli, he's comatose. If the child remains in a deep sleep and is responsive only to vigorous and repeated stimulation, he's stuporous. If the child has limited spontaneous movement and sluggish speech, he's lethargic.
8. A client with left-sided heart failure complains of increasing shortness of breath and is agitated and coughing up pink-tinged, foamy sputum. The nurse should recognize these as signs and symptoms of
A.right-sided heart failure.
B.acute pulmonary edema.
C.pneumonia.
D.cardiogenic shock.
A B C D
B
Because of decreased contractility and increased fluid volume and pressure in clients with heart failure, fluid may be driven from the pulmonary capillary beds into the alveoli, causing pulmonary edema. In right-sided heart failure, the client exhibits hepatomegaly, jugular vein distention, and peripheral edema. In pneumonia, the client would have a temperature spike, and sputum that varies in color. A client in cardiogenic shock would show signs of hypotension and tachycardia.
9. The nurse brings a new mother her neonate for the first time approximately 1 hour after the neonate's birth. After checking the identification, the nurse hands the neonate to the mother. Within a few minutes, the mother begins to undress her neonate. Which of the following should the nurse do?
A.Call the pediatrician and report the behavior.
B.Anticipate and support the behavior as a normal part of bonding.
C.Encourage the mother to rewrap the neonate because the room is cold.
D.Take the neonate back to the nursery and recheck the neonate's temperature.
A B C D
B
The behavior demonstrated by the mother is normal during the "taking-hold" process. The nurse should anticipate and support this behavior. Because this is normal behavior for establishing a relationship, it doesn't need to be reported. It's highly doubtful that the neonate would become chilled during this brief time of being undressed. Therefore, rewrapping the neonate and taking her back to the nursery to check her temperature isn't necessary.
10. During the assessment stage, a client with schizophrenia leaves his arm in the air after the nurse has taken his blood pressure. His action shows evidence of
A.somatic delusions.
B.waxy flexibility.
C.neologisms.
D.nihilistic delusions.
A B C D
B
The correct answer is waxy flexibility, which is defined as retaining any position that the body has been placed in. Somatic delusions involve a false belief about the functioning of the body. Neologisms are invented meaningless words. Nihilistic delusions are false ideas about self, others, or the world.
11. Which statement about fluid replacement is accurate for a client with hyperosmolar hyperglycemic nonketotic syndrome (HHNS) ?
A.Administer 2 to 3 L of IV fluid rapidly.
B.Administer 6 L of IV fluid over the first 24 hours.
C.Administer a dextrose solution containing normal saline solution.
D.Administer IV fluid slowly to prevent circulatory overload and collapse.
A B C D
A
Regardless of the client's medical history, rapid fluid resuscitation is critical for maintaining cardiovascular integrity. Profound intravascular depletion requires aggressive fluid replacement. A typical fluid resuscitation protocol is 6 L of fluid over the first 12 hours, with more fluid to follow over the next 24 hours. Various fluids can be used, depending on the degree of hypovolemia. Commonly prescribed fluids include dextran (in cases of hypovolemic shock), isotonic normal saline solution and, when the client is stabilized, hypotonic half-normal saline solution.
12. During a late stage of acquired immunodeficiency syndrome (AIDS), a client demonstrates signs of AIDS-related dementia. The nurse should give the highest priority to which nursing diagnosis?
A.Bathing or hygiene self-care deficit.
B.Ineffective cerebral tissue perfusion.
C.Dysfunctional grieving.
D.Risk for injury.
A B C D
D
In a client with AIDS, deterioration of the central nervous system (CNS) can lead to AIDS-related dementia. Because this type of dementia impairs cognition and judgment, it places the client at risk for injury. Although self-care deficit and dysfunctional grieving can be associated with AIDS, they don't take precedence for a client with AIDS-related dementia. Because CNS deterioration results from infection--not altered tissue perfusion--Ineffective cerebral tissue perfusion isn't an appropriate diagnosis.
13. The nurse is teaching a client recently diagnosed with myasthenia gravis. The nurse should teach the client that myasthenia gravis is caused by
A.genetic dysfunction.
B.upper and lower motor neuron lesions.
C.decreased conduction of impulses in an upper motor neuron lesion.
D.a lower motor neuron lesion.
A B C D
D
Myasthenia gravis is characterized by a weakness of muscles, especially in the face and throat, caused by a lower neuron lesion at the myoneural junction. It isn't a genetic disorder. A combined upper and lower neuron lesion generally occurs as a result of spinal injuries. A lesion involving cranial nerves and their axons in the spinal cord would cause decreased conduction of impulses at an upper motor neuron.
14. A physician schedules an invasive procedure for a client with acquired immunodeficiency syndrome-related dementia. He lives with his male companion, who is present. His mother, who lives in another state, is also present. The nurse anticipates that the consent form should be signed by
A.the companion.
B.the mother.
C.the client.
D.two physicians.
A B C D
B
The mother should sign the consent form because she's the closest living relative. The client can't sign because of his diagnosis. The companion, although a close significant other, can't sign because he isn't a blood relative. Two physicians need not sign a consent form when a relative is available.
15. A 33-year-old male client is admitted with an exacerbation of ulcerative colitis. The nurse is performing an admission assessment and assessing the teaching needs regarding appropriate diet and lifestyle modifications for the client. To develop an effective teaching plan, the nurse must solicit which of the following input from the client?
A.Details about his childhood phobias.
B.His feelings, beliefs, and attitudes about his chronic illness.
C.Information about his financial status.
D.Information about his relationship with his wife.
A B C D
B
Assessment data should include information regarding the client's feelings, beliefs, and attitudes about his illness. Although the other options are partially correct, option B is the best answer.
16. Following coronary artery bypass grafting, a client begins having chest "fullness" and anxiety. The nurse suspects cardiac tamponade and prints a lead Ⅱ electrocardiograph (ECG) strip for interpretation. In looking at the strip, the change in the QRS complex that would most support her suspicion is
A.narrowing complex.
B.widening complex.
C.amplitude increase.
D.amplitude decrease.
A B C D
D
Fluid surrounding the heart such as in cardiac tamponade, suppresses the amplitude of the QRS complexes on an ECG. Narrowing or widening complexes and amplitude increase aren't expected on the ECG of an individual with cardiac tamponade.
17. What is the most appropriate nursing diagnosis for the client with acute pancreatitis?
A.Deficient fluid volume.
B.Excess fluid volume.
C.Decreased cardiac output.
D.Ineffective gastrointestinal tissue perfusion.
A B C D
A
Clients with acute pancreatitis commonly experience deficient fluid volume, which can lead to hypovolemic shock. The volume deficit may be caused by vomiting, hemorrhage (in hemorrhagic pancreatitis), and plasma leaking into the peritoneal cavity. Hypovolemic shock would cause a decrease in cardiac output. Tissue perfusion would be altered if hypovolemic shock occurred, but this wouldn't be the primary nursing diagnosis.
18. Following a fall from a horse during rodeo practice, an 18-year-old client is seen in the emergency department. He has a large, dirty laceration on his leg. The wound is vigorously cleaned, closed, and dressed. In the past, the client has received the full immunization regimen for tetanus toxoid. The nurse asks the client about his tetanus immunization history and he says, "I had my last shot when I was 11 years old. " The nurse should
A.advise the client to get a tetanus vaccine within 3 years.
B.request the physician to order a serum tetanus titer.
C.plan on administering a dose of tetanus vaccine.
D.teach the client that he has life-long immunity to tetanus.
A B C D
C
If a client has a wound contaminated with soil that may contain animal excrement and he has completed the full childhood tetanus immunization regimen, he should be given a dose of tetanus toxoid if it has been 5 or more years since the most recent dose. (It had been 7 years since the client's last dose. ) Serum tetanus titer levels aren't used to determine whether tetanus toxoid should be administered. No available tetanus immunization confers life-long immunity.
19. A female neonate delivered by elective cesarean birth to a 25-year-old mother weighs 3,265g (7 lb, 3 oz). The nurse places the neonate under the warmer unit. In addition to routine assessments, the nurse should closely monitor this neonate for which of the following?
A.Temperature instability due to type of birth.
B.Respiratory distress due to lack of contractions.
C.Signs of acrocyanosis.
D.Unstable blood sugars.
A B C D
B
The squeezing action of the contractions during labor enhances fetal lung maturity. Neonates who aren't subjected to contractions are at an increased risk for developing respiratory distress. The type of birth has nothing to do with temperature or glucose stability, and acrocyanosis is a normal finding.
20. Which of the following statements should be included when teaching clients about monoamine oxidase (MAO) inhibitor antidepressants?
A.Don't take prescribed or over-the-counter medications without consulting the physician.
B.Avoid strenuous activity because of the cardiac effects of the drug.
C.Have blood levels screened weekly for leukopenia.
D.Don't take with aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs).
A B C D
A
MAO inhibitor antidepressants when combined with a number of drugs can cause life-threatening hypertensive crisis. It's imperative that a client checks with his physician and pharmacist before taking any other medications. Activity doesn't need to be limited. Blood dyscrasias aren't a common problem with MAO inhibitors. Aspirin and NSAIDs are safe to take with MAO inhibitors.
21. When caring for a client with preeclampsia, which action is a priority?
A.Monitoring the client's labor carefully and preparing for a fast delivery.
B.Continually assessing the fetal tracing for signs of fetal distress.
C.Checking vital signs every 15 minutes to watch for increasing blood pressure.
D.Reducing visual and auditory stimulation.
A B C D
D
A client with preeclampsia is at risk for seizure activity because her neurologic system is overstimulated. Therefore, in addition to administering pharmacologic interventions to reduce the possibility of seizures, the nurse should lessen auditory and visual stimulation. Although the other actions are important, they're of a lesser priority.
22. Which action should the nurse include in a plan of care for a client with a fiberglass cast on the right arm?
A.Keep the casted arm warm with a light blanket.
B.Avoid handling the cast for 24 hours or until dry.
C.Assess pedal and posterior tibial pulses every 2 hours.
D.Assess movement and sensation in the fingers of the right hand.
A B C D
D
The nurse should assess a casted arm every 2 hours for finger movement and sensation to ensure that the cast isn't restricting circulation. To reduce the risk of skin breakdown, the nurse should leave a casted arm uncovered to allow for air circulation through the cast pores to the skin below. Unlike plaster casts, fiberglass casts dry quickly and can be handled without damage soon after application. The nurse should assess the brachial and radial pulses distal to the cast--not the pedal and posterior tibial pulses, which are found in the legs.
23. The nurse is working in a support group for clients with acquired immunodeficiency syndrome (AIDS). Which point is most important for the nurse to stress?
A.Avoiding the use of illicit drugs and alcohol.
B.Refraining from telling anyone about the diagnosis.
C.Following safer-sex practices.
D.Telling potential sex partners about the diagnosis, as required by law.
A B C D
C
AIDS clients must follow safer-sex practices to prevent transmission of the human immunodeficiency virus. Although avoiding the use of alcohol and illicit drugs is helpful, the most important point the nurse can make is that drug users can best avoid transmission by using clean needles and disposing of used needles. The AIDS client has no legal obligation to tell anyone about an AIDS diagnosis.
24. A 21-year-old client with a history of ulcerative colitis is hospitalized for an exacerbation. When planning dietary teaching, the nurse should recommend that the client consume
A.high-protein foods, such as eggs, meat, and cheese.
B.whole milk and other dairy products.
C.raw fruits and vegetables.
D.products containing caffeine.
A B C D
A
Clients with ulcerative colitis should be encouraged to consume foods high in protein and calories to promote healing. Fat intake should be limited, especially if steatorrhea is present. Clients should also be encouraged to avoid raw fruits and vegetables, dried fruit and beans, whole grains, bran, seeds, and nuts to reduce bowel movements. Caffeine-containing and carbonated beverages should be avoided because they stimulate intestinal peristalsis.
25. A client with Hashimoto's thyroiditis and a history of two myocardial infarctions and coronary artery disease is to receive levothyroxine (Synthroid). Because of the client's cardiac history, the nurse would expect that the client's initial dose for the thyroid replacement would be which of the following?
A.25 g/day, initially.
B.100 g/day, initially.
C.Delayed until after thyroid surgery.
D.Initiated before thyroid surgery.
A B C D
A
Elderly clients and clients with cardiac disease should begin with low-dose levothyroxine increased at 2- to 4-week intervals until 100 g/d is reached. This slow titration prevents further cardiac stress. Younger clients would be started on the usual maintenance dose of 100 g/d. Clients with Hashimoto's thyroiditis don't require surgical intervention.
26. The nurse is caring for a client in acute renal failure. The nurse should expect hypertonic glucose, insulin infusions, and sodium bicarbonate to be used to treat
A.hypernatremia.
B.hypokalemia.
C.hyperkalemia.
D.hypercalcemia.
A B C D
C
Hyperkalemia, a common complication of acute renal failure, is life-threatening if immediate action isn't taken to reverse it. The administration of glucose and regular insulin, with sodium bicarbonate if necessary, can temporarily prevent cardiac arrest by moving potassium into the cells and temporarily reducing serum potassium levels. Hypernatremia, hypokalemia, and hypercalcemia don't usually occur with acute renal failure and aren't treated with glucose, insulin, or sodium bicarbonate.
27. During the admission interview, a client reports that she frequently has nightmares and memories of a rape that occurred 3 years ago. She feels depressed and asks the nurse, "Do you think I will ever get better? I don't know what is wrong with me. " The nurse's most supportive response would be
A."It sounds like you have some unresolved pain about the trauma. Take time here to talk and allow yourself to heal. "
B."I'm not sure what is wrong, but the medication will help you soon enough. "
C."It's important to talk to your physician about an issue such as this. "
D."Don't feel bad; the treatment will help you. "
A B C D
A
Option A is the most supportive statement. The nurse acknowledges the client's traumatic experience and pain as well as encourages her to talk. Option B ignores the client's need for reassurance. Option C indicates that the nurse isn't capable of helping the client deal with therapeutic issues. Option D could make the client feel guilty for being upset about the trauma.
28. Physical assessment findings in the eyes of elderly people may include
A.decreased lens thickness.
B.decreased visual acuity.
C.lightening of the skin around the orbits.
D.unequal pupillary light reflex.
A B C D
B
Decreased visual acuity is common in elderly people. Additional assessment findings include increased lens thickness and opacity, darkening of the skin around the orbits, and an equal but slowed pupillary reflex.
29. The physician prescribes several drugs for a client with hemorrhagic stroke. Which drug order should the nurse question?
A.Heparin sodium (Hep-Lock).
B.Dexamethasone (Deeadron).
C.Methyldopa (Aldomet).
D.Phenytoin (Dilantin).
A B C D
A
Administration of heparin, an anticoagulant, could increase the bleeding associated with hemorrhagic stroke. Therefore, the nurse should question this order to prevent additional hemorrhage in the brain. For a client with hemorrhagic shock, dexamethasone may be used to decrease cerebral edema and pressure; methyldopa, to decrease blood pressure; and phenytoin, to prevent seizures.
30. A client, age 59, complains of leg pain brought on by walking several blocks--a symptom that first arose several weeks ago. The client's history includes diabetes mellitus and a two-pack-a-day cigarette habit for the past 42 years. The physician diagnoses intermittent claudication and prescribes pentoxifylline (Trental), 400 mg three times daily with meals. The nurse should provide which instruction concerning long-term care?
A."Practice meticulous foot care. "
B."Consider cutting down on your smoking. "
C."Reduce your level of exercise. "
D."See the physician if complications occur. "
A B C D
A
Intermittent claudication and other chronic peripheral vascular diseases reduce oxygenation to the feet, making them susceptible to injury and poor healing. Therefore, meticulous foot care is essential. The nurse should teach the client to bathe the feet in warm water and dry them thoroughly, cut the toenails straight across, wear well-litting shoes, and avoid taking medications unless the physician approves. Because nicotine is a vasoconstrictor, this client should stop smoking, not just consider cutting down. Daily walking is beneficial to clients with intermittent claudication. The client must see the physician regularly to evaluate the effectiveness of the therapeutic regimen, not just when complications occur.
Part Two You will have one hour and 50 minutes to complete Part Two.
1. A 49-year-old client with acute respiratory distress watches everything the staff does and demands full explanations for all procedures and medications. Which of the following actions would best indicate that the client has achieved an increased level of psychological comfort?
A.Making decreased eye contact.
B.Asking to see family members.
C.Joking about the present condition.
D.Sleeping undisturbed for 3 hours.
A B C D
D
Sleeping undisturbed for a period of time would indicate that the client feels more relaxed, comfortable, and trusting and is less anxious. Decreasing eye contact, asking to see family, and joking may also indicate that the client is more relaxed. However, these also could be diversions.
2. Following a transsphenoidal hypophysectomy, the nurse should assess the client carefully for which condition?
A.Hypocortisolism.
B.Hypoglycemia.
C.Hyperglycemia.
D.Hypercalcemia.
A B C D
A
The nurse should assess for hypocortisolism. Abrupt withdrawal of endogenous cortisol may lead to severe adrenal insufficiency. Steroids should be given during surgery to prevent hypocortisolism from occurring. Signs of hypocortisolism include vomiting, increased weakness, dehydration and hypotension. After the corticotropin-secreting tumor is removed, the client shouldn't be at risk for hypoglycemia or hyperglycemia. Calcium imbalance shouldn't occur in this situation.
3. Following a cystoscopy that confirmed a diagnosis of bladder cancer, a client is scheduled for chemotherapy and a ileal conduit urinary diversion. The nurse should include which of the following points in the client's preoperative teaching?
A.The client's need to perform stoma self-care immediately after surgery.
B.The client's need to remain on bed rest for 3 days following surgery.
C.The procedure creates a stoma and he must wear a pouch afterward.
D.The client will be able to control urine passage through the stoma.
A B C D
C
The nurse should ensure that the client understands that a stoma will be formed and that he'll need to wear a pouch. The nurse will care for the stoma immediately after surgery; self-care will begin when the client is physically able. The client will be encouraged to get out of bed the first day after surgery to prevent complications of immobility. Urine flow can't be controlled through a stoma.
4. A client has been diagnosed with type A hepatitis. What special precautions should the nurse take when caring for this client?
A.Put on a mask and gown before entering the client's room.
B.Wear gloves and a gown when removing the client's bedpan.
C.Prevent the droplet spread of the organism.
D.Use caution when bringing food to the client.
A B C D
B
The nurse should wear gloves and a gown when removing the client's bedpan because the type A hepatitis virus occurs in stools. It may also occur in blood, nasotracheal secretions, and urine. Type A hepatitis isn't transmitted through the air by way of droplets. Special precautions aren't needed when feeding the client, but disposable utensils should be used.
5. An appropriate-for-gestational-age neonate should weigh
A.between the 10th and the 90th percentiles for age.
B.at least 2,500 g (5 lb, 8 oz).
C.between 2,000 and 4,000 g (4 lb, 6 oz and 8 lb, 12 oz).
D.in the 50th percentile.
A B C D
A
Appropriate-for gestational-age neonate weights fall between the 10th and the 90th percentiles for age. Large-for-gestational-age weight is above the 90th percentile, and small-for-gestational-age is below the 10th percentile for age.
6. A certified nursing assistant (CNA) is caring for a client with Clostridium difficile diarrhea and asks the charge nurse, "How can I keep from catching this from the client?" The nurse reminds the CNA to wash her hands and to ensure the client is placed
A.on protective isolation.
B.on neutropenic precautions.
C.in a negative-pressure room.
D.on contact isolation.
A B C D
D
C difficile can be transmitted from person to person by hands or waste containers such as a bedpan. When in direct contact with the client, the nurse should practice contact isolation, which includes wearing gloves and a gown. Protective isolation is used to protect a client who is immunocompromised, which isn't evident in this case. Neutropenic precautions are for clients with an absolute neutrophil count of 1,000/μL or less; this isn't evident in this case. A negative-pressure room is used when the organism is spread by the airborne route, which isn't true of C. difficile diarrhea.
7. Which behavior would cause the nurse to suspect that a client's labor is moving quickly and that the physician should be notified?
A.An increased sense of rectal pressure.
B.A decrease in intensity of contractions.
C.An increase in fetal heart rate variability.
D.Episodes of nausea and vomiting.
A B C D
A
An increased sense of rectal pressure indicates that the client is moving into the second stage of labor. The nurse should be able to discern that information by the client's behavior. Contractions don't decrease in intensity, there isn't a change in fetal heart rate variability, and nausea and vomiting don't usually occur.
8. A client complains of a severe, throbbing headache following a lumbar puncture. The priority nursing intervention for this client is to
A.restrict fluid intake.
B.increase fluid intake.
C.raise the head of the bed.
D.assess vital signs.
A B C D
B
The nurse should encourage the client to increase her fluid intake to approximately 3 qt (3 L)/day for 24 to 48 hours. The headache is most likely due to decreased cerebrospinal fluid (CSF) circulating around the cranium. This fluid loss allows the brain to move abnormally within the skull. The movement causes tension on the meninges and venous sinuses, causing pain. Extra oral fluid intake will increase CSF production. Lying flat may decrease pain, and raising the head of the bed may worsen the headache.
9. The nurse should encourage a client with a wound to consume foods high in vitamin C because this vitamin
A.restores the inflammatory response.
B.enhances oxygen transport to tissues.
C.reduces edema.
D.enhances protein synthesis.
A B C D
D
The client should be encouraged to consume foods high in vitamin C because it's essential for protein synthesis, an important part of wound healing. Hemostasis is responsible for the inflammatory response and reducing edema. Hemoglobin is responsible for oxygen transport.
10. A client's chest X-ray reveals bilateral white-outs, indicating adult respiratory distress syndrome (ARDS). This syndrome results from
A.cardiogenic pulmonary edema.
B.respiratory alkalosis.
C.increased pulmonary capillary permeability.
D.renal failure.
A B C D
C
ARDS results from increased pulmonary capillary permeability, which leads to noncardiogenic pulmonary edema. In cardiogenic pulmonary edema, pulmonary congestion occurs secondary to heart failure. In the initial stage of ARDS, respiratory alkalosis may arise secondary to hyperventilation; however, it doesn't cause ARDS. Renal failure also doesn't cause ARDS.
11. While assessing a client who complained of lower abdominal pressure, the nurse notes a firm mass extending above the symphysis pubis. The nurse suspects
A.a urinary tract infection.
B.renal calculi.
C.an enlarged kidney.
D.a distended bladder.
A B C D
D
The bladder isn't usually palpable unless it's distended. The feeling of pressure is usually relieved with urination. Reduced bladder tone due to general anesthesia is a common postoperative complication that causes difficulty in voiding. A urinary tract infection and renal calculi aren't palpable. The kidneys aren't palpable above the symphysis pubis.
12. A client with cancer undergoes a total gastrectomy. Several hours after surgery, the nurse notes that the client's nasogastric (NG) tube has stopped draining. How should the nurse respond?
A.Notify the physician.
B.Reposition the NG tube.
C.Irrigate the NG tube.
D.Increase the suction level.
A B C D
A
An NG tube that fails to drain during the postoperative period after gastrectomy should be reported to the physician immediately. The tube may be occluded, which could increase pressure on the suture line because fluid isn't draining adequately. Repositioning or irrigating the tube in a client who has bad gastric surgery can disrupt the anastamosis. Increasing the level of suction may cause trauma to GI mucosa or the suture line.
13. Which of the following would be least likely to indicate anticipated bonding behaviors by new parents?
A.The parents' willingness to touch and hold the neonate.
B.The parents' expression of interest about the size of the neonate.
C.The parents' indication that they want to see the neonate.
D.The parents' interactions with each other.
A B C D
D
Parental interaction will provide the nurse with a good assessment of the stability of the family's home life but it has no indication for parental bonding. Willingness to touch and hold the neonate, expressing interest about the neonate's size, and indicating a desire to see the neonate are behaviors indicating parental bonding.
14. The nurse inspects a client's back and notices small hemorrhagic spots. The nurse documents that the client has
A.extravasation.
B.osteomalacia.
C.petechiae.
D.uremia.
A B C D
C
Petechiae are small hemorrhagic spots. Extravasation is the leakage of fluid in the interstitial space. Osteomalacia is the softening of bone tissue. Uremia is an excess of urea and other nitrogen products in the blood.
15. A 9-month-old infant is admitted with diarrhea and deficient fluid volume. The nurse plans to assess this client's vital signs frequently. What other action would provide the most important assessment information?
A.Measuring the infant's body weight.
B.Obtaining a stool specimen for analysis.
C.Obtaining a urine specimen for analysis.
D.Inspecting the infant's posterior fontanel.
A B C D
A
Frequent assessment of weight provides important information about fluid balance and the infant's response to fluid replacement. Results of stool or urine analyses may provide information, but they're typically not available for at least 24 hours. The posterior fontanel usually closes between ages 6 and 8 weeks and therefore doesn't reflect fluid balance in a 9-month-old infant.
16. The uterus returns to the pelvic cavity in which time frame?
A.7th to 9th day postpartum.
B.2 weeks postpartum.
C.End of the 6th week postpartum.
D.When the lochia changes to alba.
A B C D
A
The normal involutional process returns the uterus to the pelvic cavity in 7 to 9 days. A significant involutional complication is the failure of the uterus to return to the pelvic cavity within the prescribed time period. This is known as subinvolution.
17. When assessing a client with chest pain, the nurse obtains a thorough history. Which statement by the client is most suggestive of angina pectoris?
A."The pain lasted for about 45 minutes. "
B."The pain resolved after I ate a sandwich. "
C."The pain worsened when I took a deep breath. "
D."The pain occurred while I was mowing the lawn. "
A B C D
D
Angina pectoris is chest pain caused by a decreased oxygen supply to the myocardium. Lawn mowing increases the cardiac workload, which increases the heart's need for oxygen and can precipitate angina. Anginal pain typically is self-limiting and lasts 5 to 15 minutes. Food consumption doesn't reduce this pain, but may ease pain caused by a GI ulcer. Deep breathing has no effect on anginal pain.
18. The nurse is assessing the puncture site of a client who has received a purified protein derivative test. Which finding indicates a need for further evaluation?
A.15-mm induration.
B.Reddened area.
C.10-mm bruise.
D.Blister.
A B C D
A
A 10-mm induration strongly suggests a positive response in this tuberculosis screening test--so, a 15-mm induration clearly requires further evaluation. The remaining options aren't positive reactions to the test and require no further evaluation.
19. A client with fecal impaction typically exhibits which clinical manifestation?
A.Liquid or semiliquid stools.
B.Hard, brown, formed stools.
C.Loss of urge to defecate.
D.Increased appetite.
A B C D
A
The passage of liquid or semiliquid stools results from seepage of unformed bowel contents around the impacted stool in the rectum. Clients with fecal impaction don't pass hard, brown, formed stools because the stool can't move past the impaction. Clients usually report the urge to defecate--although they can't pass stool--and decreased appetite.
20. The nurse applies a fetal monitor to a 15-year-old primagravida admitted to the hospital with possible pregnancy-induced hypertension. Which monitor pattern would the nurse expect to observe if the client is experiencing uteroplacental insufficiency?
A.Late deceleration.
B.Early deceleration.
C.Variable deceleration.
D.Fetal acceleration.
A B C D
A
Late deceleration is caused by uteroplacental insufficiency. Early deceleration is caused by head compression, and variable deceleration is caused by umbilical cord compression. Fetal acceleration is a sign of fetal well-being.
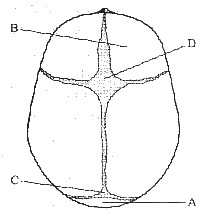
21. When assessing an infant for changes in intracranial pressure (ICP), it's important to palpate the fontanels. Where the nurse should palpate to assess the anterior fontanel?
A.A
B.B
C.C
D.D
A B C D
D
The anterior fontanel is formed by the junction of the sagittal, frontal, and coronal sutures. It's shaped like a diamond and normally measures 4 to 5 cm as its widest point. A widened,bulging fontanel is a sign of increased ICP.
22. Which of the following describes how the nurse interprets a neonate's Apgar score of 8 at 5 minutes?
A.A neonate who is in good condition.
B.A neonate who is mildly depressed.
C.A neonate who is moderately depressed.
D.A neonate who needs additional oxygen to improve the Apgar score.
A B C D
A
An Apgar score of 8 indicates that the neonate has macte a good transition to extrauterine life. A score of 4 to 6 would indicate moderate distress; a score of 0 to 3 would indicate severe distress.
23. Which of the following would be the best approach when trying to take a crying toddler's temperature?
A.Ignore the crying and screaming.
B.Encourage the mother to hold the child.
C.Talk to the mother first and then to the toddler.
D.Bring extra help so it can be done quickly.
A B C D
C
When dealing with a crying toddler, the best approach is to talk to the mother and ignore the toddler at first. This approach helps the toddler get used to the nurse before she attempts any procedures. It also gives the toddler an opportunity to see that the mother trusts the nurse. Ignoring the crying and screaming may be the second step. Having the mother hold the toddler will help if she can do this. The last resort is to bring in assistance so the procedure can be completed quickly.



 深色:已答题 浅色:未答题
深色:已答题 浅色:未答题